Original Zeng Ge Daily Popular Science Zeng Ge Daily Popular Science
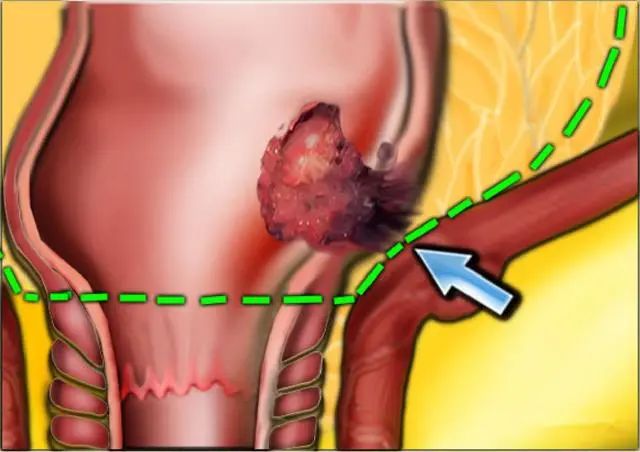
Lao Wu, 50 years old, went to the hospital for examination because of bloody stool, and found out that it was rectal cancer. To have surgery, the doctor actually asked him to lose weight first.
I did CT scan of abdomen and chest, as well as MRI scan of pelvic cavity. Fortunately, distant organs such as liver and lung did not metastasize, but pelvic MRI showed that cancer invaded the whole layer of rectal wall, and there was pelvic lymph node metastasis, so it was considered to be stage III rectal cancer.
We suggest that he do concurrent radiotherapy and chemotherapy first, which can make the tumor shrink, improve the complete resection rate, reduce the recurrence rate, and increase the probability of preserving anus. Radiotherapy can last for a long time, and it is generally recommended to rest for about 8 weeks after radiotherapy, and then do surgery.
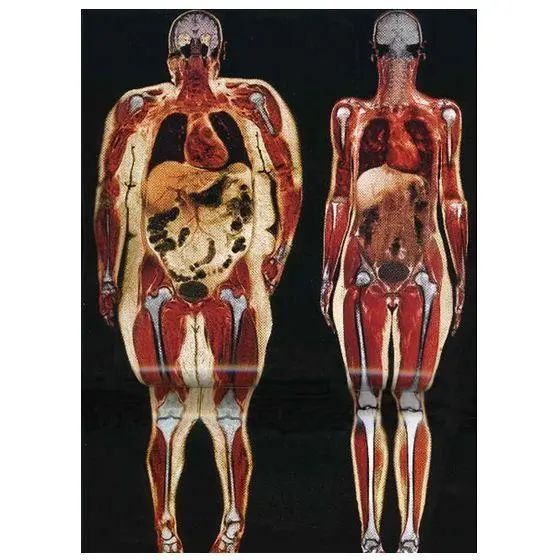
We also made a request to him, that is, during this period, he must lose weight well, because he is 170 cm tall, but his weight has reached 200 kg, and his body mass index has reached 34.6, which is seriously exceeding the standard. Moreover, Lao Wu is abdominal obesity, with a big belly and no fat arms and thighs.

Why do we let Lao Wu lose weight? Because surgeons are full of "discrimination" against fat people!
For some obese patients, surgeons often say that surgery is not easy to do, why not do it, mainly for the following reasons:
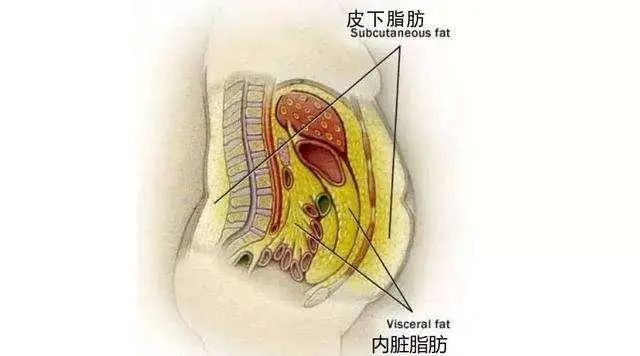
1. Obese patients have thick subcutaneous fat.
Many obese patients have a lot of stomachs. Compared with thin people, the subcutaneous fat is obviously thick. For example, the subcutaneous fat of thin people is only 0.5 cm, and that of fat people is 5 cm thick.
When doing laparotomy, the thin man will enter the abdominal cavity in a minute or two, while the fat man may take ten minutes before the doctor can cut the skin, thick subcutaneous fat, muscle and a thick layer of extraperitoneal fat, and finally enter the abdominal cavity.
When doing surgery, it is necessary to pull the abdominal wall of the patient to both sides, so as to expose the organs in the stomach, find the diseased organs or tissues, and then remove them.
We have all kinds of instruments, which are specially used to open the abdominal wall of patients. Such instruments are called retractor.

Obviously, the thin belly is easier to pull open, while the fat belly is too thick, so the doctor in charge of pulling the hook will be very hard and need to make great efforts.
We once had a rectal cancer operation. The patient was also a fat man weighing more than 200 kilograms. Two rotating students were responsible for pulling the hook. The operation was not easy to do, and it took five hours. Two students kept pulling the hook for five hours, which exhausted them.
After the operation, a classmate said, I hate fat people! Another student is relatively fat himself. He said that he must lose weight. In case he gets sick in the future, he doesn’t want to be like this patient.

After the lesion is removed, it is necessary to close the abdominal cavity and suture the surgical incision layer by layer. The fat man’s operation and closing the abdominal cavity are also technical activities. After the suture, the patient coughs and pushes hard, which is easy to split the wound. Moreover, the blood supply of adipose tissue is not very good, which is prone to incision fat liquefaction, incision infection and incision hernia.
2. The abdominal space of obese patients is small and inconvenient to operate.
Fat people not only have a fat belly, but also have a lot of visceral fat in the abdominal cavity. The omentum and mesentery are all adipose tissues, which occupy a lot of space in the abdominal cavity, resulting in a smaller space for surgical operation.
For example, when doing rectal cancer surgery, the rectum is already in the narrow pelvic cavity. If the adipose tissue around the rectum is particularly thick, it may occupy the entire pelvic cavity. When doing surgery, it is necessary to free the mesorectum from the pelvic cavity, which is very difficult to operate.
At this time, it is easy to lead to unclear anatomical levels, easy to damage blood vessels, nerves and other organs, causing collateral damage, increasing the difficulty of surgery and increasing the incidence of complications.

Therefore, it is not only difficult for fat people to have surgery, but also the incidence of complications is high. It is not that doctors discriminate against obese people. It is indeed that the difficulty of surgery is much higher than that of thin people. It is difficult for particularly obese patients to have surgery. For your health, everyone must lose weight!
Original title: "When cancer is diagnosed, the doctor is not in a hurry to operate on the patient, but let him lose weight first. Why? 》
Read the original text